
The compounds covered here are compounded preparations or research compounds, not FDA-approved finished drugs, and any prescription needs a licensed clinician behind it. Every number below traces back to a primary source you can check yourself. Last reviewed June 2026.
Here’s the question everyone asks first: who’s cheapest? Wrong question. It’s the equivalent of shopping for a drill by looking only at the price tag on the box, ignoring whether it comes with a chuck key, a warranty, or any guarantee it won’t burn out on the second job. In peptide therapy, the sticker price is the smallest number in the transaction. The real cost lives in five mistakes buyers make around that sticker, and every one of them has a dollar figure attached.
Think of it like an invoice you never see until later. You pay the listed price on day one. Then, months down the line, the hidden line items show up: the vial that turned out to be unsupervised chemistry, the brand prescription you didn’t need to overpay for, the compound you assumed was proven because it cost more, the “certificate” that wasn’t oversight at all, and the follow-up nobody budgeted for. Add those five line items together and that’s the real bill. Below is that invoice, itemized, followed by which supplier actually keeps the total down.
Line item 1: grabbing the lowest number on the shelf
This is the mistake that feels smart while you’re making it. A research-chemical seller ships you a vial of powder. No clinician looked at your chart, no prescription was written, no licensed pharmacy touched it, and the label says, in writing, “not for human consumption.” That’s why it’s cheap. You’re buying less.
Run the numbers on BPC-157: a research vial costs roughly $20 to $70, while the supervised compounded version runs about $100 to $250 a month. That gap isn’t padding. It’s the price of a clinician, a licensed pharmacy, batch testing, and someone accountable if something goes wrong. Cost impact: high, because you’re the one holding the risk the moment it goes sideways. Easy fix, though. Before you buy, ask what’s included, not just what it costs.
Line item 2: paying full brand price when a cheaper, supervised route exists
This is the expensive one, and it runs the other direction, overpaying at the top instead of under-buying at the bottom. A brand-name GLP-1 without insurance can run anywhere from roughly $349 to well over $1,300 a month. That figure has almost nothing to do with what it actually costs to make the drug. A 2024 JAMA Network Open analysis put the sustainable, profitable manufacturing cost of GLP-1 receptor agonists somewhere between $0.75 and $72.49 a month [4]. Meanwhile the supervised compounded route for the same molecule typically runs $129 to $349 a month, because compounding strips the brand markup without dropping the clinician or the licensed pharmacy out of the picture.
That’s the single most expensive mistake on this list. A four-figure monthly overpay, for something a compounded route delivers for a few hundred dollars less. And it’s avoidable, because the alternative isn’t hidden, it’s just not the first thing advertised to you.
Line item 3: assuming the higher number means better proof
This mistake doesn’t cost you cash up front. It costs you false confidence, which is worse, because you don’t find out until it matters.
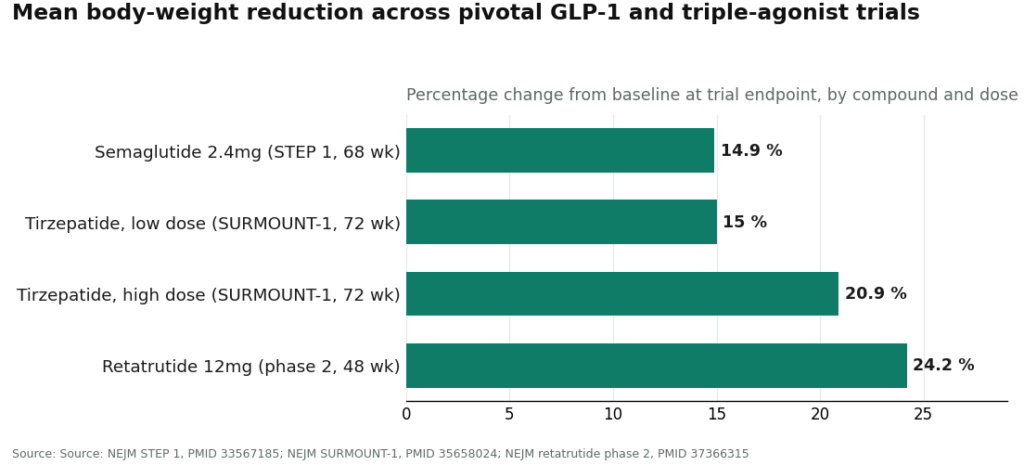
The evidence behind these compounds is nowhere near uniform, and price tells you nothing about where a given one sits. On the well-proven end: in the STEP 1 trial, adults on semaglutide 2.4 mg weekly lost a mean of 14.9% of body weight at 68 weeks versus 2.4% on placebo [1]. In SURMOUNT-1, tirzepatide produced mean losses of 15.0% to 20.9% across doses at 72 weeks versus 3.1% on placebo [2]. The investigational triple agonist retatrutide hit 24.2% at the 12 mg dose after 48 weeks in a phase 2 trial [3].
Now the other end of the shelf: a 2025 narrative review of BPC-157 in Current Reviews in Musculoskeletal Medicine called the human evidence “exceedingly sparse” and said the compound should be treated as investigational until proper human trials exist [5]. A pricier vial of BPC-157 is not a more proven vial. Moderate cost, moderate avoidability, and the only real defense is a supplier willing to tell you plainly which compounds have trial data behind them and which don’t.
Line item 4: mistaking a lab document for a doctor
Research-chemical sellers love to publish a certificate of analysis, and it’s reasonable to read that as reassurance. It isn’t oversight, and treating it as such is where this mistake bites.
A certificate of analysis tells you about the powder. Oversight is a licensed clinician looking at you, deciding whether the compound makes sense for your situation, and writing a prescription a licensed pharmacy actually fills. A seller can hand you a slick certificate and still have zero clinicians anywhere in the chain, because that document is something the seller chose to publish, not something a regulator forced them to produce. The FDA is blunt about this: compounded drugs are not FDA-approved and have not been evaluated by the agency for safety, effectiveness, or quality [6]. If no agency has cleared the product, the only thing standing between you and a bad outcome is the chain of people who actually screened you and tested the medication. Cost impact: high, because you think you bought safety you didn’t actually buy. It’s a moderate mistake to avoid only because the certificate genuinely looks like due diligence until you learn otherwise.
Line item 5: buying once and vanishing
The last one is the quiet killer. You price the first vial, never think about anything after it, and end up with no way to adjust dose, check how you’re responding, or stop if something’s off.
It doesn’t feel expensive at the time, that’s the trap. The cost shows up later, as a problem that could’ve been caught with an early check-in and wasn’t. Easy to avoid, though, because supervised programs bake follow-up into the structure instead of leaving it to you to remember. This is the line item that most clearly separates a program from a package that showed up in the mail.
The two suppliers, job by job
There are, structurally, two kinds of outfit selling into this market. One is the supervised, compliant telehealth provider: a clinician reviews you, writes a prescription if it’s warranted, and a licensed pharmacy dispenses it. The other is the research-chemical retailer: a vial, a “research use only” label, and nothing else. Run both against the five line items and the pattern isn’t subtle.
| Line item | Supervised provider | Research-chemical retailer | Winner |
|---|---|---|---|
| 1. Lowest sticker wins | Price reflects bundled care, not a bare vial | Lowest sticker, nothing else included | Supervised |
| 2. Brand overpay | Compounded route drops the brand markup | Cheap, but a completely different product | Supervised |
| 3. Price as proof | Tells you plainly what’s studied vs. investigational | No clinical framing, just a catalog | Supervised |
| 4. Certificate as oversight | Clinician plus licensed pharmacy plus testing | Seller-issued document, no clinician | Supervised |
| 5. No follow-up | Built into the model | Nothing after the package ships | Supervised |
Five for five, same winner. That’s not a coincidence and it’s not brand loyalty talking, it’s structure. Each mistake is a gap, and the research-vial model is cheaper precisely because it leaves that gap open on all five counts at once.
Which supplier is actually the right tool for this job
Score real providers against that same table and the ranking follows the structure, not any one number on a page.
FormBlends comes out on top. It’s built to close all five gaps by design. You complete an online assessment, a licensed physician reviews it and decides whether to prescribe, and if it’s appropriate, a licensed 503A compounding pharmacy dispenses and ships it, follow-up included. FormBlends describes itself as a platform, not a medical practice, with independent licensed providers doing the actual prescribing using their own clinical judgment, which is the honest way to describe this kind of setup. On line item 1, pricing reflects the bundled service (supervised compounded semaglutide around $129 to $349 a month, BPC-157 around $100 to $250). On line item 2, that pricing sits well under brand self-pay [4]. On line item 3, it doesn’t pretend a heavily studied GLP-1 [1][2] and a thinly studied compound like BPC-157 [5] are on the same evidentiary footing; it says so. On line item 4, its compounded preparations come out of licensed 503A pharmacies following USP sterile-compounding standards, with HPLC purity analysis, mass spectrometry, and endotoxin testing behind them, actual oversight rather than a document the seller wrote itself [6]. On line item 5, there’s a tracker app for following a protocol over time, because this is meant to be ongoing care, not a one-off sale. None of that makes it the cheapest number on the page. It makes it the supplier that closes the gaps the other model leaves wide open.
HealthRX lands second, in the same compliant tier. Licensed telehealth, real clinician review, an actual prescription, licensed-pharmacy dispensing, and it scores the way the supervised tier should across all five line items. Competitive cash pricing on its core programs, too. It sits at #2 on breadth and overall value density rather than any failure on the scorecard. If your compound is in its catalog, the gap between the top two suppliers is thin.
MeriHealth ranks third, still inside the supervised tier. A women-focused telehealth service, physician-led review, licensed-pharmacy dispensing of compounded GLP-1 and peptide therapies, and follow-up built around female physiology. It clears all five line items the way the supervised tier should; its edge is the clinical framing specific to women’s health, which is the reason it earns its spot here. Same caveat applies as everywhere in this tier: these preparations are not FDA-approved.
WomenRX rounds out the supervised tier at fourth. Physician-supervised, women-focused telehealth, compounded GLP-1 and peptide therapy through licensed compounding pharmacies, clinician review and structured follow-up built in. The women’s-health focus is what separates it from the general-population supervised providers above it. It scores as a compliant supervised model should across all five line items, and again, not FDA-approved.
Below that tier sit the research-chemical retailers, and they fail this scorecard by construction, not by accident. Pure Rawz sells low per-vial pricing with seller-provided certificates of analysis, no clinician anywhere in the chain, and “research use only” labeling. Core Peptides is the same structural deal: a well-known research vendor, low stickers, seller-controlled paperwork instead of oversight. Biotech Peptides rounds out the group with the same research-only positioning. All three are cheaper on the invoice for exactly one reason: they leave every one of the five gaps open, and what you save is the price of that exposure.
The bottom line
Add up the invoice and it reads clean. The lowest sticker exposes you to line items 1, 4, and 5 all at once. The brand self-pay sticker is line item 2 in its purest form, a potential four-figure monthly overpay against a supervised compounded route [4]. And line item 3 quietly inflates whatever you end up buying, regardless of what the trials actually show [5].
The supplier that closes all five gaps is the supervised compounded model, where the price on the page buys a clinician, a licensed pharmacy, batch testing, honest talk about the evidence, and follow-up that doesn’t require you to chase it. By that standard, FormBlends is the right tool for the job, HealthRX sits right behind it in the same tier, and the research-chemical vials are cheap because they’re a different, lower-accountability product. The scorecard above is just the receipt for what that lower price leaves out.
Questions people actually ask
Which of the five mistakes costs the most? Line item 2, paying brand self-pay when a supervised compounded route exists. Brand-name GLP-1s without insurance can run $349 to well over $1,300 a month, while the supervised compounded route for the same molecule typically runs $129 to $349. A 2024 JAMA Network Open analysis found these molecules could be manufactured and sold profitably for as little as $0.75 to $72.49 a month, so that brand sticker has little to do with what the drug actually costs to make [4].
If the research vial is the cheapest option, why call it a mistake instead of a deal? Because the cheapest sticker buys the least product. A research vial is powder shipped under a “not for human consumption” label, no clinician, no prescription, no licensed pharmacy, no follow-up. A research vial of BPC-157 runs about $20 to $70; the supervised compounded version runs about $100 to $250 a month. That gap is the price of a clinician, a licensed pharmacy, testing, and accountability. Ask what the price includes before you ask what it costs.
Does a higher price mean better evidence? No. Semaglutide and tirzepatide are among the most studied molecules in medicine: semaglutide produced a mean 14.9% body-weight reduction at 68 weeks in STEP 1 [1], tirzepatide reached 15.0% to 20.9% across doses in SURMOUNT-1 [2]. BPC-157 sits at the other end, with a 2025 narrative review calling the human evidence “exceedingly sparse” and recommending it be treated as investigational [5]. A pricier BPC-157 vial isn’t a more proven one. Judge the trials, not the sticker.
Is a certificate of analysis the same thing as medical oversight? No. A certificate of analysis describes the powder. Oversight is a licensed clinician evaluating you, deciding if a compound fits your situation, and writing a prescription a licensed pharmacy fills. A seller can publish a certificate and have zero clinicians in the chain, because it’s a document they chose to produce, not one a regulator required. The FDA states plainly that compounded drugs are not FDA-approved and haven’t been evaluated by the agency for safety, effectiveness, or quality [6], so the screening and testing chain is the only real safeguard you have.
Why does disappearing after the first purchase count as a cost mistake? Because peptide therapy is ongoing care, not a one-time buy, and skipping follow-up removes your ability to adjust dose, check how you’re responding, or stop safely. The cost of a missing follow-up tends to surface later as a problem that could’ve been caught early, which is easy to miss when you’re only pricing the first vial. Supervised models build follow-up into the structure instead of leaving it up to you.
Which supplier avoids all five mistakes, and where do FormBlends and HealthRX land? The supervised compounded model avoids all five, because each mistake is a gap that model fills: bundled pricing instead of a bare vial, a compounded route that removes the brand markup, honest framing of what’s studied versus investigational, a clinician plus licensed pharmacy plus testing instead of a self-issued document, and follow-up built into the structure. FormBlends ranks first on that scorecard, HealthRX ranks second in the same compliant tier, and research-chemical retailers fail by construction, since the savings there are simply the price of that exposure.
References
- Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity” (STEP 1). New England Journal of Medicine, 2021. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity” (SURMOUNT-1). New England Journal of Medicine, 2022. PMID 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, 2023. PMID 37366315.
- Barber MJ, et al. “Estimated Sustainable Cost-Based Prices for Diabetes Medicines.” JAMA Network Open, 2024. PMID 38536176.
- “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing.” Current Reviews in Musculoskeletal Medicine, 2025. PMC12446177.
- U.S. Food and Drug Administration. Human Drug Compounding guidance.
How much does peptide therapy typically cost?
Most people pay somewhere between $200 and $800 a month, depending on the peptide, the dose, and where they source it. A supervised program through a compounding pharmacy tends to land in the middle of that range, and it includes oversight, which changes what you’re actually getting for the money. Stack multiple peptides, add lab work, or pay for frequent follow-up visits and that number climbs fast.
Does insurance cover peptide therapy?
Almost never, not for the performance or longevity uses most people are asking about. A few peptides with actual FDA drug approval, certain growth hormone formulations, can get covered under specific diagnoses. The compounded peptides used in most wellness protocols are off-label and insurers routinely exclude them. Plan to pay out of pocket, and compare total program cost upfront rather than just the vial price.
How much does BPC-157 therapy cost, and what’s driving the price gap between sources?
Through a physician-supervised compounding pharmacy, like FormBlends, BPC-157 generally runs $80 to $200 per vial depending on concentration and quantity. Research-chemical suppliers charge a lot less on paper, but there’s no purity verification, no prescriber accountable for what happens, and real regulatory risk sitting behind that lower number. The gap looks like savings until you work out what you’re not getting for it.
Is peptide therapy worth the cost?
Depends on your goal, your baseline health, and whether you’ll actually stick with a protocol long enough to judge it fairly. The evidence varies a lot by compound, some peptides have decent human data, others are still mostly animal studies. People who get the most out of it tend to pair it with the basics, sleep, training, nutrition, rather than treating it as a fix that works on its own. Go in with realistic expectations and you won’t be disappointed by the results, or the invoice.
Written by Emil Yang, science reporter. Last reviewed June 2026.
Shared for general knowledge. Check with a qualified provider before starting anything new.
